A first-ever global study finds massive inequity of access to and quality of health care among and within countries, and concludes people are dying from causes with well-known treatments.
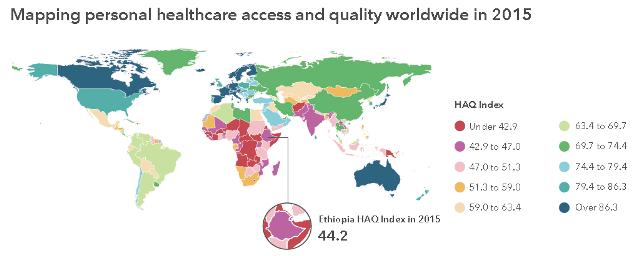
Ethiopia has improved significantly over the past 25 years, increasing its rating of 23 in 1990 to 44 in 2015, based on an index of 0 to 100, according to a research paper published in the international medical journal, The Lancet.
Ethiopia’s current health care system ranks high in addressing diphtheria, a common vaccine-preventable disease, with a score 89, as well as Hodgkin’s lymphoma with a score of 92. However, in other categories the nation had much lower scores, such as in tuberculosis (score of 20), and neonatal disorders (score of 21).
The study is the first effort to assess access and quality of services in 195 countries. Researchers used a Healthcare Access and Quality (HAQ) Index, based on death rates from 32 causes that could be avoided by timely and effective medical care, known as “amenable mortality.”
The top-ranked nation was Andorra with an overall score of 95; its lowest treatment score was for Hodgkin’s lymphoma at 70. The lowest ranked nation was Central African Republic at 29; its highest treatment score was for diphtheria at 65.
“What we have found about health care access and quality is disturbing,” said Dr. Christopher Murray, senior author of the study and Director of the Institute for Health Metrics and Evaluation (IHME) at the University of Washington. “Having a strong economy does not guarantee good health care. Having great medical technology doesn’t either. We know this because people are not getting the care that should be expected for diseases with established treatments.”
For example, Norway and Australia each scored 90 overall, among the highest in the world. However, Norway scored 65 in its treatment for testicular cancer, and Australia scored 52 for treating non-melanoma skin cancer.
“In the majority of cases, both of these cancers can be treated effectively,” Dr. Murray said. “Shouldn’t it cause serious concern that people are dying of these causes in countries that have the resources to address them?”
Scores were based on estimates from the annual Global Burden of Diseases, Injuries, and Risk Factors study (GBD), a systematic, scientific effort to quantify the magnitude of health loss from all major diseases, injuries, and risk factors by age, sex, and population. With more than 2,300 collaborators in 133 countries, the GBD examines 300-plus diseases and injuries.
In addition, data were extracted from the most recent GBD and evaluated using a Socio-demographic Index (SDI) of rates of education, fertility, and income. SDI goes beyond the historical “developed” versus “developing” nations. Similar previous studies were limited primarily to high income countries, particularly in Western Europe.
Nations in much of sub-Saharan Africa, as well as in Asia and the Pacific, experienced the lowest rankings. Nonetheless, many countries in these regions, including China (score: 74) and Ethiopia (score: 44), have seen sizeable gains since 1990.
The paper does offer some favorable signs of improvement in health access and quality. Since 1990, several countries achieved progress that met or surpassed levels reached by other nations of similar development. These countries included Turkey, Jordan South Korea, the Maldives, Niger, Jordan, and several Western European nations such as Switzerland, Spain, and France.
IHME plans each year to update the report, “Healthcare Access and Quality Index Based on Mortality from Causes amenable to personal Healthcare in 195 Countries and Territories, 1990 – 2015: A Novel Approach to the Global Burden of Disease 2015 Study.” It aims to use these results to better understand gaps and opportunities for improving health access throughout the world.
The Healthcare Access and Quality (HAQ) Index is a summary measure based on 32 causes, that in the presence of high-quality healthcare, should not result in death. These 32 causes were selected as part of research that Professor McKee and Dr. Ellen Nolte, both co-authors in this study, began in the early 2000s.
The causes are: Tuberculosis, Diarrhea-related diseases, Lower respiratory infections, Upper respiratory infections, Diphtheria, Whooping cough, Tetanus, Measles, Maternal disorders, Neonatal disorders, Colon and rectum cancer, Non-melanoma skin cancer, Breast cancer, Cervical cancer, Uterine cancer, Testicular cancer, Hodgkin lymphoma, Leukemia, Rheumatic heart disease, Ischemic heart disease, Cerebrovascular disease (stroke), Hypertensive heart disease, Chronic respiratory diseases, Peptic ulcer disease, Appendicitis, Inguinal, femoral, and abdominal hernia, Gall bladder and biliary diseases, Epilepsy, Diabetes, urogenital, blood, and endocrine diseases, Chronic kidney disease, Congenital anomalies, Adverse effects of medical treatment
Ethiopia’s Healthcare Access and Quality Profile
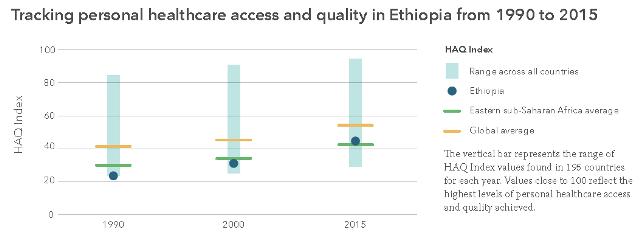
Monitoring national levels of personal healthcare access and quality is critical to understanding where countries can improve health service delivery. Researchers used findings from the Global Burden of Disease (GBD) study to estimate a summary measure of healthcare access and quality, the Healthcare Access and Quality (HAQ) Index, for 195 countries from 1990 to 2015.
Based on the relationship between countries’ HAQ Indices and overall socio-demographic development, researchers charted an HAQ Index “frontier,” or the highest access and quality countries achieved at different development levels. Key results for Ethiopia are highlighted here, while all results can be found at bit.ly/amenable-mortality.
Key results on personal healthcare access and quality
* Globally, personal healthcare access and quality, as measured by the HAQ Index, improved from 40.7 in 1990 to 53.7 in 2015, on a scale of 0 to 100. For Ethiopia, personal healthcare access and quality increased from 23.1 in 1990 to 44.2 in 2015.
* Despite overall gains in personal healthcare access and quality, the gap between the highest and lowest levels increased from 1990 to 2015. Among countries in the same GBD region as Ethiopia (Eastern sub-Saharan Africa), 2015 HAQ Index values ranged from 34.2 in Somalia to 49.9 in Tanzania.
* Given a country’s resources and development, the gap between its HAQ Index and frontier represents how much untapped potential exists for improving personal healthcare access and quality.
* Globally, the gap was 20.1 in 2015, changing minimally since 1990. For Ethiopia, this gap was 13.7 in 1990 and 3.9 in 2015, reflecting progress in improving healthcare access and quality alongside gains in development.
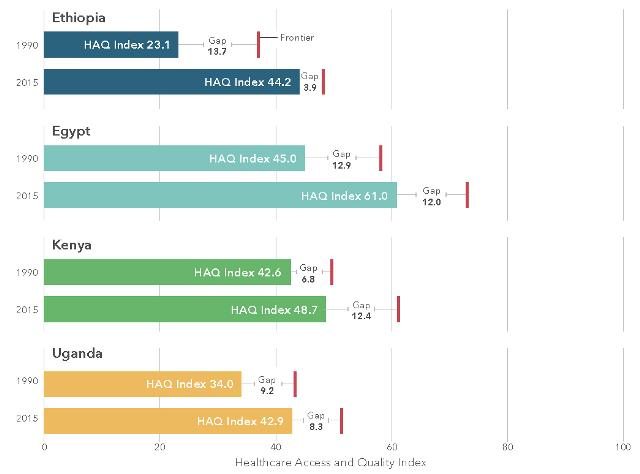
Understanding the gap between a country’s HAQ Index and what could have been achieved (the HAQ Index frontier), given its socio-demographic development, has major policy implications. This gap highlights the untapped potential for improving healthcare based on a country’s current resources.
Where this gap is small or exceeds levels achieved by countries of similar development, opportunities may exist for advancing healthcare access and quality with gains in development. A large or growing gap could be viewed as a warning sign that improved healthcare access and quality is not an inevitable result of increased development. This figure shows changes in the HAQ Index frontier gap for Ethiopia and three comparator countries.
Definitions
Healthcare Access and Quality (HAQ) Index Provides a summary measure of personal healthcare access and quality for a given location. This measure is based on risk-standardized mortality rates from causes that, in the presence of high-quality healthcare, should not result in death – also known as amenable mortality.
HAQ Index Frontier
Represents the highest personal healthcare and access achieved at a given level of development. The difference between a country’s HAQ Index and its frontier is the “gap.”
**********
Source: GBD 2015 Healthcare Access and Quality Collaborators. Healthcare Access and Quality Index based on mortality from causes amenable to personal healthcare in 195 countries and territories, 1990–2015: a novel analysis from the Global Burden of Disease 2015 study. The Lancet. 2017 May 18.






Comments are closed.
Leave a Comment